The world of mental health care increasingly relies on a structured approach to patient assessment and treatment. One such approach is the Soap Notes Counseling Template, a powerful tool for clinicians to effectively document patient interactions, analyze data, and inform treatment plans. This template provides a framework for capturing crucial details, promoting consistency, and facilitating a deeper understanding of the patient's experience. It's more than just a form; it's a strategic tool designed to enhance the quality of care delivered. Soap Notes Counseling Template is a vital component of modern therapeutic practice, enabling clinicians to move beyond simple observation and towards a more holistic and insightful assessment. Its adaptability allows it to be tailored to various specialties and clinical settings, making it a versatile resource for practitioners of all disciplines. This article will delve into the core components of the Soap Notes Counseling Template, exploring its benefits, practical implementation, and how it can be utilized to improve patient outcomes.
Understanding the Core Principles
At its heart, the Soap Notes Counseling Template is built on the principle of detailed and chronological documentation. It emphasizes capturing not just what happened during a session, but how it felt, why it happened, and the patient's subjective experience. This holistic approach is crucial for identifying patterns, understanding underlying issues, and developing targeted interventions. The template encourages clinicians to move beyond a purely diagnostic mindset and instead, to actively engage with the patient's narrative. It's about building a collaborative partnership, fostering trust, and empowering the patient to take ownership of their care. The template's structure is designed to minimize ambiguity and maximize clarity, ensuring that all relevant information is readily accessible. It's a system, not just a checklist, and consistent application is key to its effectiveness.

Section 1: Initial Patient Information
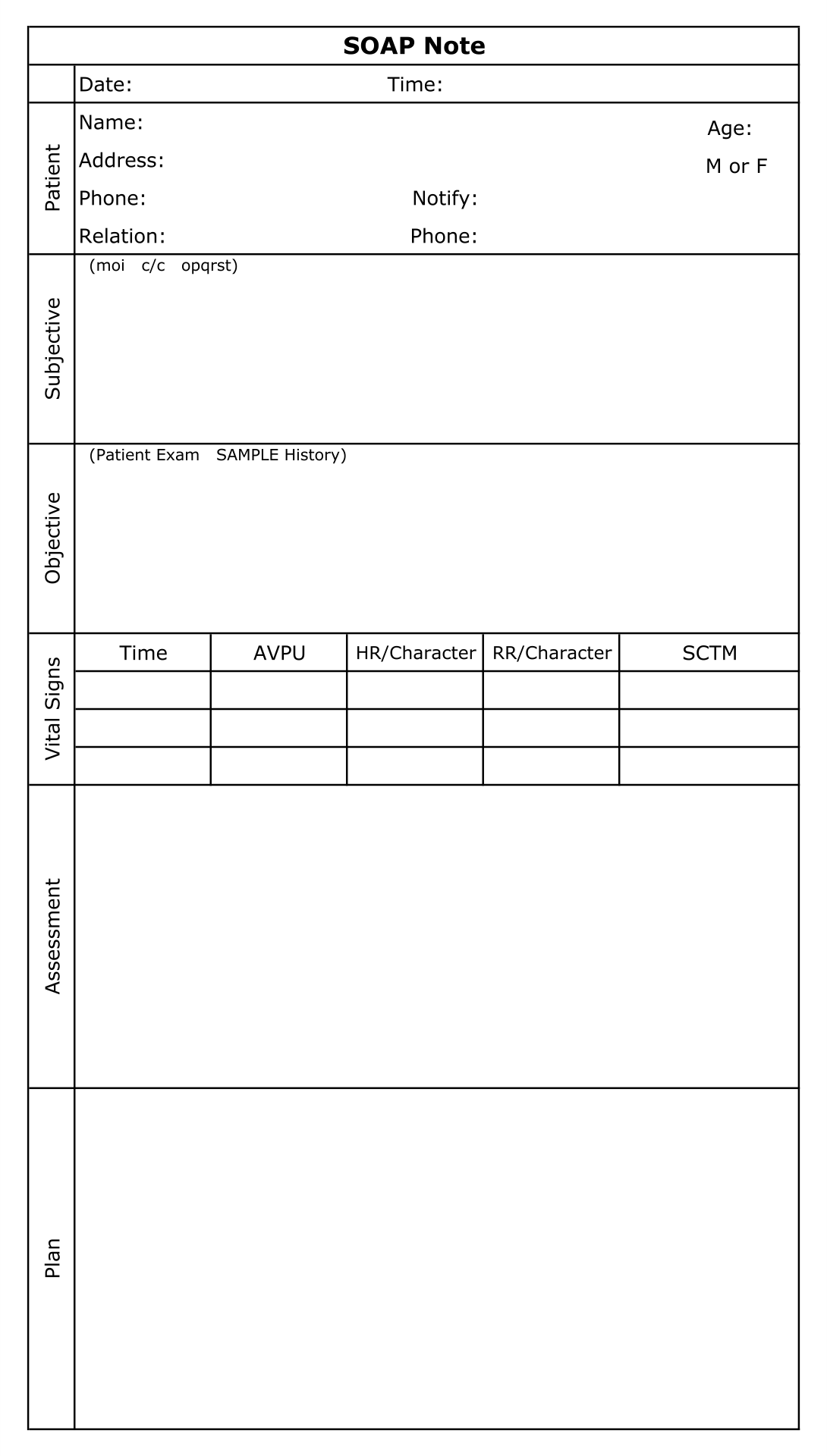
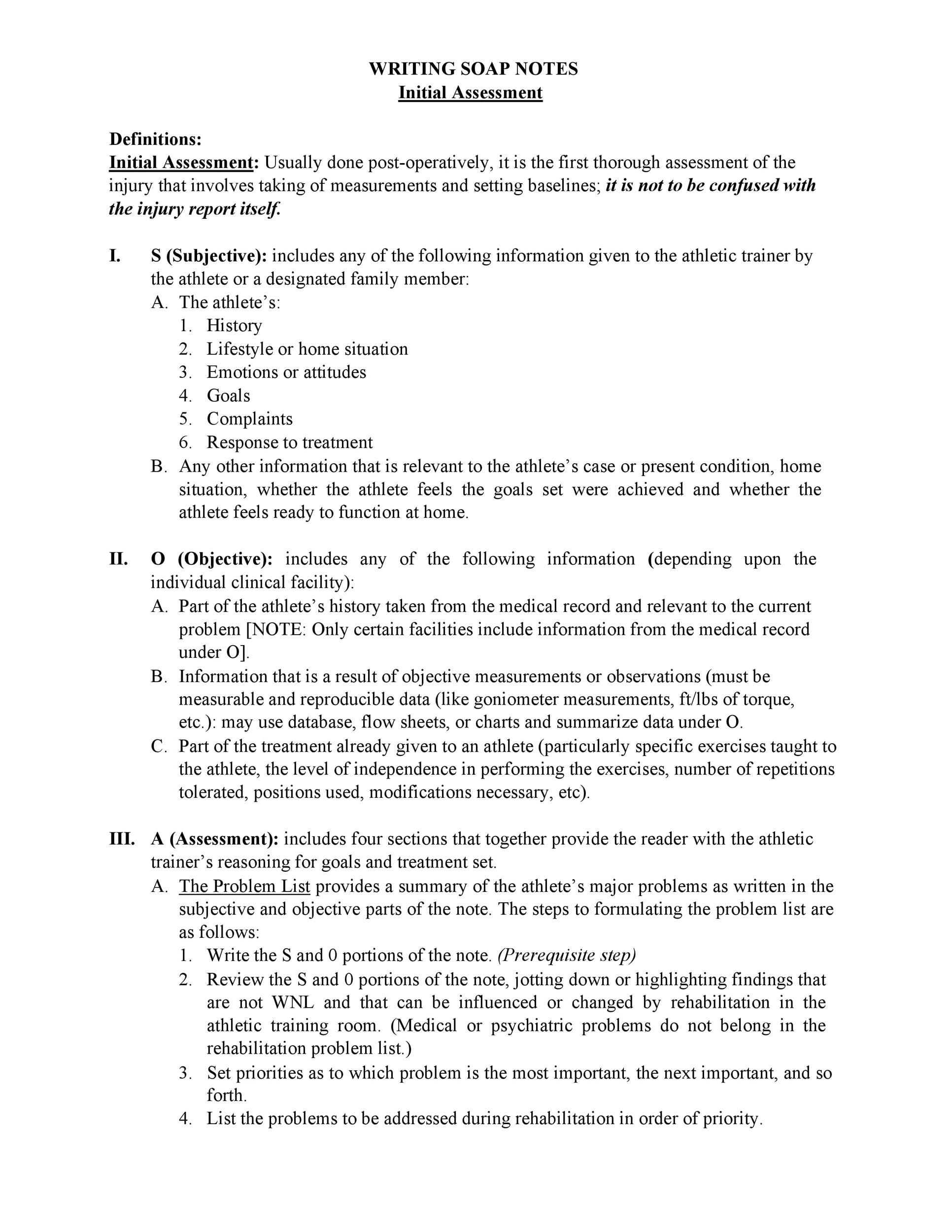
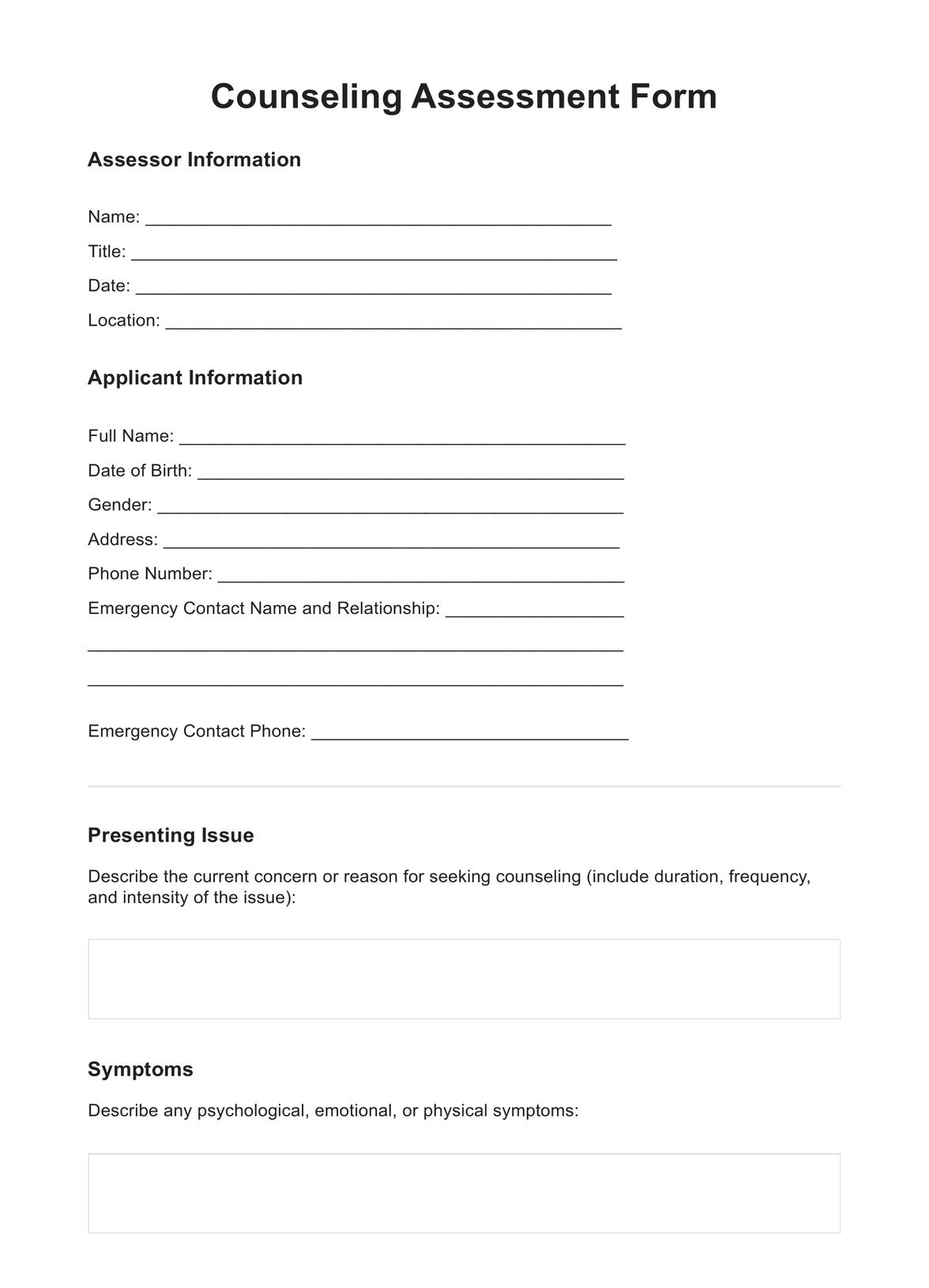
The first section of the template is dedicated to gathering essential patient information. This includes details such as the patient's demographic information (name, age, gender, contact details), current diagnosis, treatment plan, and any relevant medical history. It's vital to ensure this information is accurate and up-to-date. For example, the template should include fields for the patient's primary diagnosis, secondary diagnoses, and any co-occurring conditions. Collecting this foundational data allows for a more comprehensive understanding of the patient's situation. Furthermore, documenting the patient's current level of distress or engagement is crucial. This can be achieved through a brief assessment of their emotional state and their willingness to participate in the session. This initial assessment provides a baseline for monitoring progress throughout the treatment process.
Section 2: Session Summary – Key Events and Observations
This section is the core of the template, detailing the key events and observations that occurred during the session. It's structured chronologically, allowing clinicians to easily follow the patient's journey. Each event should be described using clear, concise language, focusing on the patient's perspective. For instance, instead of simply stating "Patient reported feeling anxious," the description should include details like "Patient expressed feelings of worry and apprehension regarding their upcoming surgery." It's important to note any significant changes in the patient's behavior, mood, or physical state during the session. This section also includes a brief assessment of the patient's coping mechanisms and any challenges they may be facing. This section is particularly important for identifying potential triggers and developing appropriate interventions.
Exploring the Patient's Narrative
A critical element of this section is encouraging the patient to share their own story. The template should include prompts designed to elicit the patient's perspective, such as "Can you tell me about what happened during our session?" or "What was the most important thing you experienced today?" It's crucial to create a safe and supportive environment where the patient feels comfortable sharing their thoughts and feelings. Active listening is paramount – clinicians should focus on truly understanding the patient's experience, rather than simply waiting for their turn to speak. The template should also incorporate techniques for probing deeper into the patient's narrative, such as asking open-ended questions and using reflective listening.

Section 3: Assessment and Diagnostic Impressions
This section focuses on the clinician's assessment of the patient's condition and the diagnostic impressions formed during the session. It's a space for clinicians to articulate their observations, including any relevant symptoms, behaviors, or thoughts. The template should include a structured approach to assessment, such as using a standardized rating scale or a checklist to capture key indicators. For example, the template might include sections for assessing mood, anxiety levels, cognitive functioning, and physical symptoms. It's important to avoid making definitive diagnoses at this stage, but rather to provide a preliminary assessment based on the patient's presentation. The clinician should also document any relevant diagnostic criteria or hypotheses that are being considered.
Identifying Contributing Factors
A significant aspect of this section is identifying the factors that may be contributing to the patient's current challenges. This could include social stressors, relationship difficulties, trauma, or underlying medical conditions. The template should encourage clinicians to consider a range of potential contributing factors, rather than focusing solely on the immediate problem. For example, the clinician might note that the patient's anxiety is related to a recent job loss and a strained relationship with their partner. This level of detail can be invaluable for developing a comprehensive treatment plan.
Section 4: Treatment Plan and Interventions
This section outlines the treatment plan that is being implemented, including specific interventions and goals. It's a crucial section for ensuring that all treatment goals are aligned and that the patient's needs are being met. The template should include a clear statement of the treatment goals, such as "To reduce anxiety levels and improve coping skills." It should also outline the specific interventions that are being used, such as cognitive behavioral therapy (CBT) techniques, relaxation exercises, or medication management. The template should also document the patient's progress towards these goals, including any measurable outcomes. Regular monitoring and adjustments to the treatment plan are essential for ensuring that the patient is receiving the most effective care.
Section 5: Additional Notes and Observations
This final section provides a space for clinicians to record any additional notes or observations that are relevant to the patient's case. This could include information about the patient's family dynamics, social support system, or any other factors that may be influencing their recovery. It's important to be thorough and to capture all relevant details, even if they seem insignificant at first glance. This section is particularly useful for identifying potential barriers to recovery and developing strategies to address them. It also allows for a more holistic view of the patient's overall well-being.
Conclusion
The Soap Notes Counseling Template is a valuable tool for clinicians seeking to improve the quality of patient care. Its structured format, emphasis on detailed documentation, and focus on patient-centered communication contribute to a more effective and therapeutic experience. By consistently utilizing this template, clinicians can capture crucial information, promote consistency, and ultimately improve patient outcomes. The template's adaptability allows it to be tailored to a wide range of clinical settings and specialties. It's a cornerstone of modern therapeutic practice, empowering clinicians to provide compassionate and effective care. Ultimately, the effectiveness of the template hinges on its consistent and thoughtful application, requiring clinicians to prioritize patient needs and to view each session as an opportunity for collaboration and growth. The continued evolution of this template, incorporating feedback and incorporating new therapeutic approaches, will undoubtedly remain a vital resource for mental health professionals for years to come.
0 Response to "Soap Notes Counseling Template"
Posting Komentar